I recently had the honor of presenting the keynote at the Behavioral Health Initiative Wellness Day hosted by the Wisconsin Office for the Deaf and Hard of Hearing. It was an environment designed with the Deaf and hard of hearing community in mind—focused on our wellness and our unique communication needs.
But as I reflected on the event, I couldn’t shake a concerning story shared by a fellow participant who was recently asked to bring their own interpreter to a doctor’s appointment. This wasn’t an isolated incident of "old school" thinking; it mirrored my own experience. While scheduling a telehealth appointment, a nurse asked me: "Do you have someone at home who is going to sign for you?"
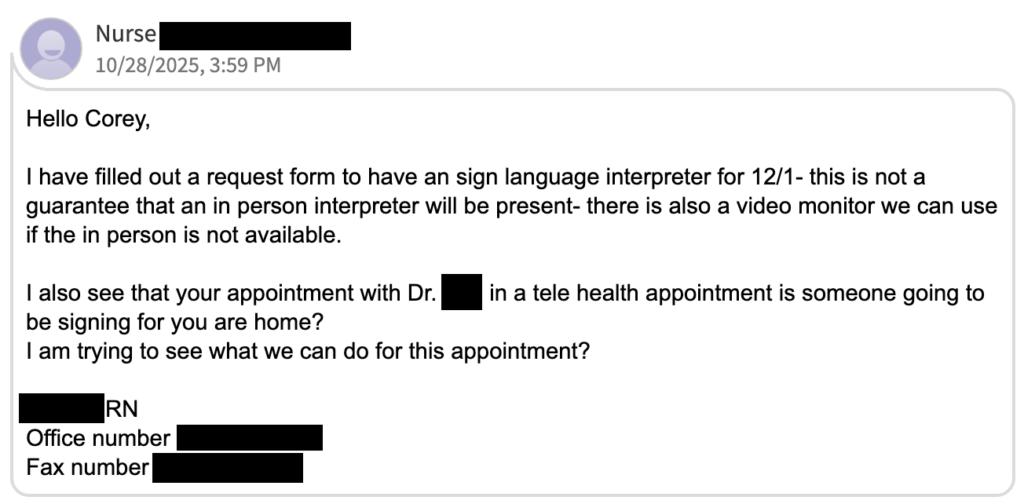
In 2026, despite leveraging AI and technology, healthcare organizations are still shifting the burden of communication onto the patient. Case in point, this recent experience left me forced to explain basic legal access to a representative of an organization ranked by U.S. News & World Report for "excellence in care."
The Analogy: Providing Your Own Infrastructure
Imagine walking into a hospital for a broken leg. The triage nurse looks at you and says, "We can fix that, but we’re short on supplies today. Did you happen to bring your own X-ray machine? Also, if you need surgery, you’ll need to provide your own anesthesia."
You would be horrified. You would likely report them for malpractice. Why? Because an X-ray and anesthesia aren't "perks"—they are the fundamental infrastructure required for the hospital to do its job.
For a Deaf or hard of hearing individual, effective communication is fundamental. Much like anesthesia, the procedure, diagnosis, and treatment plan cannot be safely executed without it. When a clinic asks me to bring my own interpreter or “just use my phone” for captions, they aren't asking for a favor; they are admitting they lack the basic infrastructure to treat me.
The Myth of the "Sovereign" Accommodation
We must stop using the word "accommodation" when the patient provides it. If someone is forced to "make do" by lip-reading or engineering their own access via a personal phone and a voice-to-text app, that is not an accommodation—these subpar workarounds are survival tactics.
True accommodations are the responsibility of the covered entity. When a hospital relies on a patient’s family or expects them to provide their own hardware and software to communicate, they aren’t being "accommodating"; they are being negligent. They are effectively telling the patient, "Your right to understand your own health is only valid if you do the labor to make it happen."
The Danger of the Waiver
Perhaps the most concerning trend is the pressure on patients to "waive" their right to effective communication. We’ve all been there: the waiting room is full, the doctor is rushed, and you just want to get the appointment over with. You think, "I'll just wing it this time."
But every time we "wing it," we reinforce a dangerous precedent. We give healthcare systems a pass to remain inaccessible. We accept a lower standard of care—one where we might miss a dosage instruction or a nuance in a diagnosis—that a hearing person would never be asked to tolerate.
AI: A Tool, Not a Patch or Replacement
We live in an era where AI is marketed as a universal bridge, capable of translating text to speech and sign to text in real-time. But in a clinical setting, we must be careful not to mistake a convenience tool for a qualified professional.
AI lacks the cultural competency, medical nuance, and ethical accountability of a certified interpreter or a professional captioner. High-tech should never be used as a "get out of jail free" card for providers to lower their standards of care. When a hospital relies solely on a tablet or an algorithm to facilitate life-altering conversations, they are choosing a lower-cost "patch" over a stable foundation. Innovation should enhance our access, not provide an excuse to dismantle the professional standards that keep patients safe.
Moving Forward
Healthcare organizations must remember that "effective communication" is a clinical requirement, not a logistical suggestion. The interpreter is as fundamental to the room as the electricity and the running water.
To my fellow Deaf and hard of hearing community members: your right to a provider-funded access solution is not a "favor" you are asking of the system. It is a right you are owed. You shouldn't have to be the architect, the contractor, and the laborer just to get through the front door.
When you pull out your own phone to run a captioning app just to understand a diagnosis, you are providing the hospital’s infrastructure for them. We need to stop bringing our own "oxygen" to the appointment. It’s time the hospitals started providing the air.